Innovation in small cell lung cancer (SCLC) and other high-grade neuroendocrine cancers (NECs)
A POWERFUL CONNECTION
Delta-like ligand 3 (DLL3)-targeted investigational immunotherapy: harnessing the potential of T cells to fight SCLC1
Unlocking the Potential of T-Cell Engagers & DLL3 in SCLC
0:01Narrator 1: What we see tells a story, whether it’s gazing toward the heavens at worlds we can only imagine, or looking inward, finding answers locked inside the tiniest of containers. When we cast our eyes on something new for the first time, how we see it, what we decide to do with what we see, is as important as what we see. We see possibilities. We see opportunity. We see hope. Like picking out constellations in the ancient sky, discovering galaxies that are farther away than we knew existed, or peering into a microscope to see the body at work at the smallest scale.
0:50Narrator 1: We connect the dots to create powerful connections, and we tell a new story. We share that story with the world. We try to make the world better. Today begins a new journey to explore the potential of targeting DLL3 in SCLC with an investigational T-cell engager technology. Join us as we dive into this technology and SCLC.
1:23Narrator 2: Please welcome Dr Sumita Bhatta and Dr Jason Porter.
1:29Dr Sumita Bhatta: Thank you all for joining us today! We are excited to be here, live from Brooklyn, to bring you an exciting topic for discussion and education. We're here tonight to dive into a few different areas that all have to do with small cell lung cancer, a devastating disease. Innovation will also be a topic for today's webcast—specifically, innovation around T-cell engager technology; what exactly is it, how it is designed to work, and what could it mean for the potential future of small cell lung cancer treatment? Before we begin, let me go ahead and introduce myself, and of course, our key speaker today.
2:05Dr Sumita Bhatta: My name is Sumi Bhatta, and I am the Vice President of Medical Affairs for oncology at Amgen. And, with us today is Dr Jason Porter. Dr Porter is a medical oncologist and hematologist at the West Cancer Center and Research Institute in Memphis, Tennessee where he also serves as the Director of the Lung Cancer Disease Research Group.
2:25Dr Jason Porter: Thank you, Sumi. I’m really excited to be here tonight, and to discuss the topic with you of small cell lung cancer!
2:33Dr Sumita Bhatta: Now, this program is being presented on behalf of Amgen Inc., the sponsor of this program, and has been reviewed consistent with Amgen’s internal review policies. This is an educational presentation and it is not intended to promote Amgen products or any other product. Further, it should not be construed as a representation that any specific therapy might be safe or effective at treating any particular disease. Also, please note this presentation is not a CME-accredited program.
3:02Dr Sumita Bhatta: Lastly, though we're together virtually, we'd love to engage with you all through the chat feature! Throughout this program we will be putting some questions and polls up for the audience, so please feel free to submit any questions or comments through the discussion using the Q&A feature! We will be answering them at the last portion of this webcast. Let’s test the polling feature now and learn more about those who have tuned in! The first question for you is what type of healthcare provider are you? Choose A for oncologist, B for nurse practitioner, C for Physician assistant, D for nurse, E for Pharmacist, or F for other. I'll give it a few seconds to await the polling results. Thanks so much for responding. It looks like the majority of you answered “other” and we do have a fair amount of pharmacists and oncologists on the line.
4:04Dr Sumita Bhatta: Now as a follow up question for you all, do you treat patients with small cell lung cancer in your practice? Please answer A for yes and B for no. Still waiting for some of those numbers to come in.
4:27Dr Sumita Bhatta: Now it's looking actually like the majority of you have answered “no”, but a fair number, about a third have answered “yes” as well. So let's go ahead and dive in. Small cell lung cancer is an aggressive high-grade neuroendocrine cancer with rapid growth and early metastases. It is a less common form of lung cancer, making up approximately 10 to 15% of all lung cancers.
4:52Dr Sumita Bhatta: In 2023, it is estimated that there will be about 30,000 new cases of small cell lung cancer in the United States. This is in contrast to an estimated 195,000 new cases of non-small cell lung cancer. And while small cell lung cancer is less common, it is quite devastating, with patients facing poor long-term outcomes and poor quality of life with this disease. With this in mind, Dr Porter, can you tell us more about the unmet need for patients with this disease?
5:21Dr Jason Porter: Absolutely. As you just mentioned, small cell lung cancer is an aggressive disease. It can present as limited-stage or extensive-stage disease, which depends on if the cancer has spread and to where. Limited-stage disease usually refers to cancer that is confined to one side of the chest—cancer that is in one lung and sometimes also the lymph nodes on the same side of the chest. Extensive-stage disease refers to cancer that has spread further across the lung, to the opposite lung, or to other areas of the body. About two-thirds of patients already have extensive-stage disease at diagnosis, presenting with significant symptoms such as cough, dyspnea, and maybe even hemoptysis. And unfortunately, while the disease initially responds to treatment, most patients will progress within months.
6:13Dr Jason Porter: The 5-year relative survival for invasive small cell lung cancer hasn’t changed much over the past few decades, and it’s only around 7%. Extensive-stage disease has an especially poor prognosis, with a median survival being only about 10 to 13 months. Smoking is a predominant risk factor for small cell lung cancer. Of course, other risk factors are out there and they can include COPD, air pollution, radon exposure, and genetics. Due to the strong association with smoking, small cell lung cancer has a high rate of molecular alterations. But interestingly, there are no actionable biomarkers to treat the disease.
6:50Dr Sumita Bhatta: Thank you so much, Dr Porter. Audience, here's another polling question for you—what percentage of your patients with small cell lung cancer are diagnosed with extensive-stage disease? Choose A for less than 20%, B for 20 to 40%, C for 40 to 60%, D for 60 to 80%, and E for greater than 80%. And while we're waiting for those responses, Dr Porter, maybe I'll ask you a question. Tell me a bit about the patients you see in your practice. What proportion of them have small cell lung cancer and how do they usually present to you?
7:25Dr Jason Porter: Right. So in my practice, I'm actually kind of selected to see patients with small cell lung cancer. So I see about 25% of patients with small cell; that's a little bit higher than our national average which runs around 13%. But those patients can come in with no symptoms at all from you know having no symptoms. They can have shortness of breath. They may come with cough if the disease is spread to other areas of the body such as bone or brain, they may have bone pain or you know, neurologic symptoms such as seizures or altered mental status at the time of presentation. And you really get everything from zero to 100.
8:02Dr Sumita Bhatta: You know our poll has suggested that the percentage of patients with small cell lung cancer that are diagnosed with extensive disease is between 60% and 80%. And I think Dr Porter, you'll tell us whether that's right, what percentage is diagnosed with extensive-stage disease in your practice?
8:17Dr Jason Porter: Usually it's about 75%. So 3/4 of them, it's very uncommon to find limited-stage disease because right now there's no standard screening for small cell lung cancer. All of our screening protocols are really geared towards non-small cell lung cancer.
8:31Dr Sumita Bhatta: So now going back to the discussion, it's clear that there's significant unmet medical need for patients with small cell lung cancer. How has the treatment landscape evolved over time, Dr Porter?
8:43Dr Jason Porter: Hardly at all honestly. So over the last few decades there have been only a few treatment advances for small cell lung cancer. The standard-of-care for extensive-stage disease remained platinum-based chemotherapy until only very recently. In 2019 and 2020, two anti–PD-L1 checkpoint inhibitors in combination with platinum-based chemotherapy were FDA-approved for first-line, extensive-stage disease. And while immune checkpoint inhibitors have significantly changed the treatment paradigms across multiple other cancer types, it has been limited success in small cell lung cancer. There have been limited advancements beyond the first-line setting as well. There were two FDA-approved therapies in second line, one of which was only approved in 2020. And, there is no established standard-of-care in or after the third-line setting. But there have been ongoing efforts to drive innovation in the space, starting with learning more about the disease biology and pathophysiology, and where is yet to be still much uncovered. Research suggests that small cell lung cancer may be stratified into four biologic subtypes, but it remains largely heterogeneous disease. All that is to say, there remains a high unmet need for patients with this disease.
9:59Dr Sumita Bhatta: Yes—we need innovation for patients with small cell lung cancer. Speaking of innovation, let’s ask the audience what they have heard! Have you, audience, heard about any investigational targets in small cell lung cancer? Please answer A for yes and B for no. And while you're answering, Dr Porter, I have another question for you. You had mentioned that there really aren't approved therapies in the third-line setting. So what in practice do you offer to your patients
10:25Dr Jason Porter: All right, so we're going with that aggressive first-line therapy, platinum doublet, plus an anti–PD-L1 or PD-L1 therapy. And then in second line we have two chemotherapy options. As we mentioned, one was only recently approved. In the third-line space, what I end up doing is something that's not standard, there's no FDA-approved therapy. So I may go back and do platinum chemotherapy again if it's been a long time since they had it. But many times, hospice is the only option that I have for those patients. They may not have other options or they may not be able to tolerate what's out there.
10:54Dr Sumita Bhatta: Yeah, it reflects that the high unmet need. So let's go back to the polling question and see how you've all answered. When the question was, have you heard about investigational targets in small cell lung cancer, 69% answered yes and around 35% answered no. So now let's ask another question, which investigational targets in small cell lung cancer have you heard of? Please select all that apply. Answer A for PARP, B for ATR kinase, C for MYC, D for Other, and E for None. We'll give it a few seconds to see the responses… Looks like there's a pretty even split between PARP and MYC, but what's really taking the cake here is the other category… I'm just waiting to see if this poll stabilizes, but now it looks pretty good. So we've got MYC, PARP, and ATR kinase that has been heard of, but there is something there in the other category. So, let me ask you a question, Dr Porter. There has been some excitement in the field regarding the potential of delta-like ligand 3, or DLL3, as a target. Audience, are you familiar with DLL3 as an emerging target? Please answer A for yes and B for no.
12:20Dr Sumita Bhatta: And with that, Dr Porter, I want to reflect on a story that you had shared with me a bit earlier. In 2018 you were at ASCO and you had showed me a contemplative selfie that you had taken of yourself. Can you share with us what were you thinking about during that time?
12:34Dr Jason Porter: All right. So in 2018 we were hearing more and more about ALK, EGFR, and different targeted therapies in non-small cell lung cancer. And I left ASCO that year thinking what about small cell, where are the targets? And I actually started looking it up and doing my own research, a deep dive, and I found DLL3, which had some therapies that were in investigation at that time, early phase, like phase one. And I started to look and dig and on that picture; I was actually sitting there thinking about DLL3 and ways to target in different combinations of therapies that we may be able to use. I didn't hear much about it except for a couple of drugs that really didn't make it that far until recently. And I've been really excited to hear what's happening in DLL3 now.
13:15Dr Sumita Bhatta: And so going back to the poll, more than half of our audience is familiar with DLL3 as an emerging target. So with that, Dr Porter, can you tell us a little bit more about DLL3?
13:26Dr Jason Porter: Sure. So, well, much is still unknown about the biological function of DLL3. However, we know that it is an inhibitory protein of Notch signaling, a pathway that’s involved in embryonic development and neuroendocrine cell differentiation. DLL3 has been implicated in tumorigenesis and tumor progression of neuroendocrine cancers. In small cell lung cancer, it has also been shown to promote migration and invasion.
13:54Dr Sumita Bhatta: So what makes DLL3 a potential target?
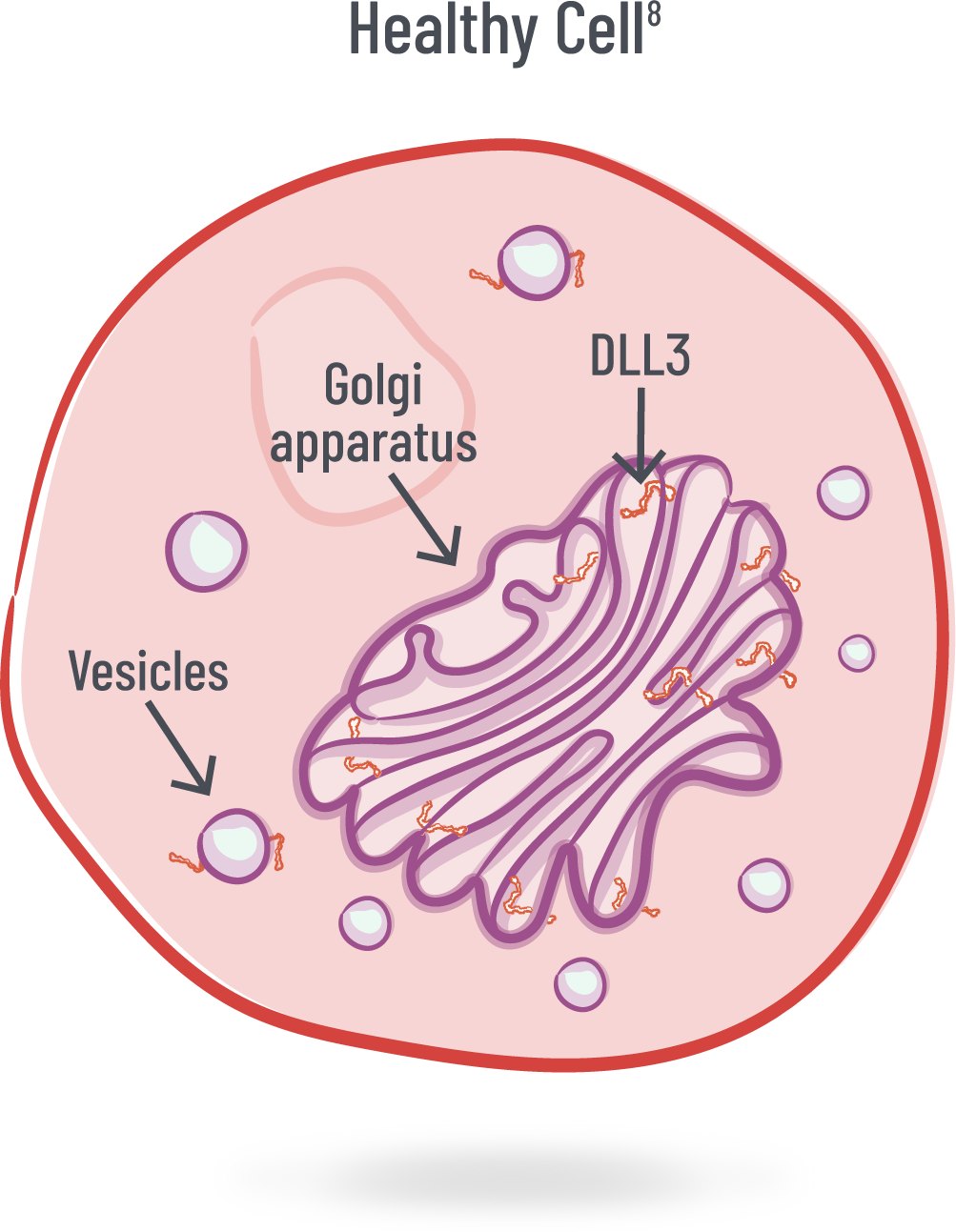
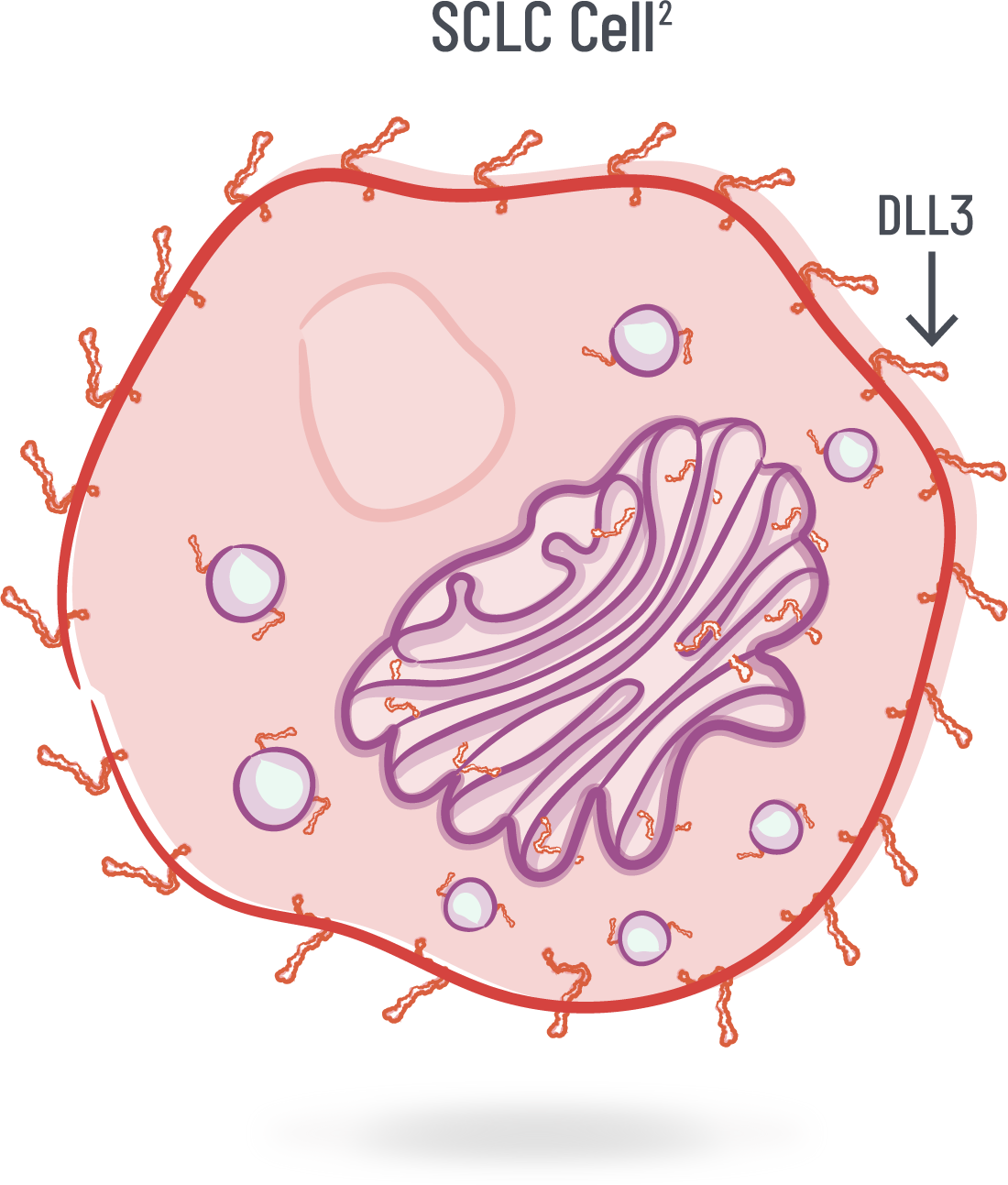
13:58Dr Jason Porter: Well, in healthy cells, DLL3 is minimally expressed and typically located in the Golgi apparatus and cytoplasmic vesicles, and is rarely found on the cellular surface. But DLL3 is highly expressed in high-grade neuroendocrine cancers like small cell lung cancer. In oncology, our goal is to treat the cancer cells, while minimizing the effect on normal cells. And so, a target, such as a protein, has potential if it’s more highly expressed in tumor tissue than in healthy tissues.
14:29Dr Sumita Bhatta: Interesting. Audience, let’s test our knowledge a bit. How prevalent do you think DLL3 expression is among patients with small cell lung cancer? Answer A for less than 20%, B for 20 to 40%, C for 40 to 60%, D for 60 to 80%, and E for greater than 80%. I'm going to give it a few seconds, wait on a couple more responses…and I'm going to report out the results. So it looks like there's pretty much a near even split between 40 to 60% and greater than 80%, with a third of the audience members expecting that DLL3 expression in lung cancer may be on the order of 20 to 40%. So Dr Porter, can you tell us how prevalent DLL3 expression is among patients with small cell lung cancer?
15:44Dr Jason Porter: Sure, so actually, it’s about 85% of patients with small cell lung cancer that express DLL3. This was studied in a large, multicenter study of 1,050 patients with small cell lung cancer, where DLL3 positivity was based on immunohistochemical staining of at least 25% of tumor cells. DLL3 staining was considered present if the tumor cells showed punctate and/or diffuse cytoplasmic and/or partial or circumferential membranous staining.
16:13Dr Sumita Bhatta: And tell us, does the prevalence remain consistent across stages and across lines of therapy?
16:20Dr Jason Porter: Yes, so in the same study we just reviewed, they observed that 83% of patients with limited-stage disease and 86% of patients with extensive-stage disease had positive DLL3 expression. The proportion of patients with positive DLL3 expression remained consistently high across lines of therapy, ranging from 83 to 89%.
16:41Dr Sumita Bhatta: That is consistently high. And what do we know about the prognostic implications of DLL3? Is DLL3 a prognostic indicator?
16:49Dr Jason Porter: So, interestingly, research shows that it may be a prognostic indicator in some neuroendocrine cancers. But DLL3 expression does not appear to be a prognostic indicator in small cell lung cancer. In this same study we just reviewed, no difference in median survival was observed among patients with or without DLL3 expression. Even among patients with positive DLL3 expression, there was no difference in survival based on degree of positivity. Nonetheless, DLL3 is a potential target due to its high expression in small cell lung cancer.
17:23Dr Sumita Bhatta: I see, so this high expression in small cell lung cancer and minimal expression in normal cells makes DLL3 seem like an exciting potential target, especially for investigational T-cell engager technology.
17:35Dr Sumita Bhatta: Now before we dive into the discussion on T-cell engager technology, here we have another question for the audience: Audience, are you familiar with T-cell engagers in the oncology space? Please answer A for yes and B for no. All right. Still giving it a couple of seconds. We need some Jeopardy music in here, don't we, Dr Porter?
18:05Dr Jason Porter: I will sing it for you, but I don't want you to put me off stage.
18:08Dr Sumita Bhatta: I know you have a talent for music. While we're waiting, Dr Porter, you had mentioned to me that you knew very early on that you wanted to be a doctor. I know you said that St Jude's inspired the oncology element of it, but what inspired the doctor part?
18:23Dr Jason Porter: Well, I don't know. I was in Memphis and I had a granddaddy who had prostate cancer and some gastric cancer and other things that I have been exposed to really early. But I knew St Jude was there and I always wanted to be a pediatric oncologist. With time in medical school, I decided adult oncology and because my dad had small cell lung cancer, I decided thoracic oncology. And so that's what I'm doing now and I love it.
18:46Dr Sumita Bhatta: Yeah, you're great. All right, so here are our answers. Are you familiar with T-cell engagers in the oncology space, 80% answered yes and 20% answered no. Well, that's great. So now, Dr Porter, let’s dive into the discussion on T-cell engager technology. Can you tell us what role cytotoxic T cells play in fighting cancer?
19:06Dr Jason Porter: Yes, well, cytotoxic T cells play an important role in recognizing and fighting tumor cells. They recognize cancer cells via T-cell receptor-major histocompatibility complex I or MHC I binding. This occurs when MHC I molecules on the cell surface of tumor cells present antigens, which the T-cell receptors are able to recognize, and ultimately result in T-cell–mediated tumor cell lysis. But tumors can often evade the immune detection by several mechanisms. And these can include downregulation of MHC I complex, inhibition of the T-cell receptor signaling, use of PD-1 or PD-L1 signaling pathways, and the formation of an immunosuppressive tumor microenvironment. And what’s important to understand is that small cell lung cancer is known as being an immunologically “cold tumor” with few infiltrating cytotoxic T cells. In fact, approximately 80% of small cell lung cancer tumors may be immunologically “cold.” There are several factors within that tumor microenvironment that may contribute to this—these can include the extracellular matrix, chemokines, and infiltration of immunosuppressive cells.
20:19Dr Sumita Bhatta: Well interesting because this is where investigational T-cell engagers could have potential since they're designed to direct cytotoxic T cells to target tumors. Audience, have you heard about investigational T-cell engagers in the small cell lung cancer landscape? Please answer A for yes and B for no. And while we're waiting for that response, Dr Porter, you had mentioned that small cell lung cancer is immunologically cold. Could you explain a little bit more about what it means to be cold?
20:46Dr Jason Porter: Right. So whenever there is a cancer present, infection, viruses, bacteria, the inflammatory response involves the influx of immune system cells that can fight against whatever that foreign invader is, whether it's the infection or cancer cells. Unfortunately, when we look at small cell tumors, often the immune system cells haven't kind of influxed into that tumor to cause the inflammatory response that can be anti-cancer. And so we call that a cold tumor. There are some subtypes of small cell and one is called inflamed and that's one where we can see immune checkpoint inhibitors being sometimes more active.
21:22Dr Sumita Bhatta: All right, so looking at the polling question, it looks like maybe folks are not sure about investigational T-cell engagers in the small cell lung cancer landscape. So would you mind telling us a little bit more about them?
21:34Dr Jason Porter: Sure! So, T-cell engagers are currently being investigated for the treatment of small cell lung cancer. And they’re designed to direct the patient's own T cells to target a tumor-associated antigen on those tumor cells, without relying on normal T-cell receptor-MHC I recognition. Once T-cell engager molecules bind both a tumor-associated antigen, such as DLL3, on tumor cells and CD3 on T cells, they create an immunological synapse, with the goal of activating T cells. Once the T cells are activated, they create perforin pores in the tumor cell membrane, allowing for the transfer of granzymes, which may induce apoptosis of the tumor cell. Activated T cells also proliferate, resulting in the expansion of T cells to potentially facilitate additional T-cell–dependent killing.
22:25Dr Sumita Bhatta: Thank you for providing that helpful overview, I can see the imagery in my mind. Audience, do you know about Bispecific T-cell Engager, or BiTE®, technology? Please answer A for yes or B for no. We'll give it a few seconds. Wait for the responses to populate. All right. This might be another one where a little bit of explanation would be very helpful. So Dr Porter, how are BiTE® molecules designed?
23:01Dr Jason Porter: Sure. A Bispecific T-cell Engager, or BiTE® molecule, consists of two single chain variable fragment domains that are designed to bind a tumor-associated antigen on tumor cells and CD3 on T cells. Some also include a silenced Fc domain which extends the half-life of the molecule.
23:22Dr Sumita Bhatta: OK, so BiTEs® are basically another form of T-cell engagers.
23:28Dr Jason Porter: Right, right. So BiTEs®, another way of targeting different tumor-associated antigens, are being investigated in both hematologic and solid tumor malignancies. This field is still growing and expanding, so much is yet to be uncovered.
23:44Dr Sumita Bhatta: Audience, this is very exciting. I have another question for you all. Overall, how exciting does T-cell engager technology seem for the advancement of the small cell lung cancer landscape? Please answer A for very exciting, B for moderately exciting, C for not exciting, and D for need more information. And Dr Porter, I'm coming to you next for your opinion on this question. As soon as we get the audience a chance to populate their responses on the live poll…we'll have to ensure that the polling function is functioning. But let us just go ahead to your answer, how excited are you about T-cell engager technologies?
24:33Dr Jason Porter: I'm really excited about any technology that’s going to move us forward in small cell lung cancer. We already talked about it being a treatment desert where we really don't have a lot of therapies out there, especially beyond second line. So this bispecific T-cell engager technology is really using a patient's own immune system to try to fight against the cancer, which may give a more sustainable response for patients who do respond. So I'm really excited about the technology and also the potential of the therapy as it's being developed.
25:02Dr Sumita Bhatta: That's great. And so I would like to ask you, Dr Porter, as we close out this portion of the discussion, do you have anything else to add?
25:10Dr Jason Porter: Yes! I think it’s very important to reemphasize that small cell lung cancer is an aggressive disease with devastating outcomes. There definitely remains a need for innovative therapy for these patients.
25:24Dr Sumita Bhatta: Tell us a bit about your experience with these patients.
25:26Dr Jason Porter: So in my clinic, I get a new diagnosis of small cell lung cancer in a patient, and that patient may or may not have symptoms and they start on very aggressive first-line therapy. They usually respond very well. Unfortunately, I have to let those patients know that there's a high likelihood that that disease will eventually relapse. And in more than 80% of those patients, they do relapse. And we go on to second-line therapy, understanding that response rate may be lower and a duration of that response may be much shorter. And so for those patients, I give them a preface that they may not respond for long and that ultimately for most of them, unfortunately, it's going to be the cause of their death. So we need to develop more therapies. And DLL3 is an exciting potential target for these investigational T-cell engagers in this space, as it’s highly expressed in small cell lung cancer and minimally expressed in the normal cells. Together, I think DLL3-targeted T-cell engager technology may provide a powerful connection, redirecting those cytotoxic T cells to target and help fight small cell lung cancer.
26:30Dr Sumita Bhatta: Thank you Dr Porter, so much, for spending this time with us and educating us on small cell lung cancer and the various treatments. For more information and resources on DLL3 and investigational T-cell engager technology, we encourage you to visit dll3possibilities.com. Thank you again and thanks to everyone for tuning in to this event this evening.
26:53Narrator 2: Thanks for joining today's broadcast. To learn more about emerging targets and modalities in SCLC, please go to dll3possibilities.com. Thank you.
There remains a need for new and innovative therapies
with durable benefits for patients with SCLC6
Delta-like ligand 3 (DLL3) is an exciting potential target in SCLC2,8
DLL3 is expressed in SCLC and other high-grade NECs, but is minimally expressed or absent on the surface of healthy cells2,8
-
DLL3 is an inhibitory protein of Notch signaling, a pathway that is involved in embryonic development and neuroendocrine cell differentiation2
-
In healthy cells, DLL3 is typically located intracellularly on membranes of the Golgi apparatus and cytoplasmic vesicles, and is rarely found on the cell surface8
DLL3 expression
~ 85%–96% | of patients with SCLC
|
DLL3 expression is consistent across lines of therapy in SCLC
Prevalence of DLL3 Expression Across SCLC Lines of Therapy9
Due to its high expression in SCLC and minimal expression on the surface of healthy cells, DLL3 is a target for T-cell engager (TCE) technology5
**Based on a multicenter, international, noninterventional study of 1,050 patients with 1 specimen and evaluable DLL3 expression. DLL3 positivity was based on immunohistochemistry staining with ≥ 25% of tumor cells that expressed DLL3. DLL3 staining defined as present if tumor cells showed punctate and/or diffuse cytoplasmic and/or partial or circumferential membranous staining.9
††Based on the DeLLphi-301, phase 2, open-label study of 157 patients with ES-SCLC and an evaluable tumor-tissue sample. 151 out of 157 patients were DLL3-positive (96%). DLL3 expression was defined as detection of expression on more than 0% of tumor cells.10
1L, first line; 3L, third line; NEC, neuroendocrine cancer.
T-cell engagers designed to target DLL3 are being investigated in SCLC and other high-grade NECs5
Cytotoxic T cells may play an important role in recognizing and fighting tumor cells11
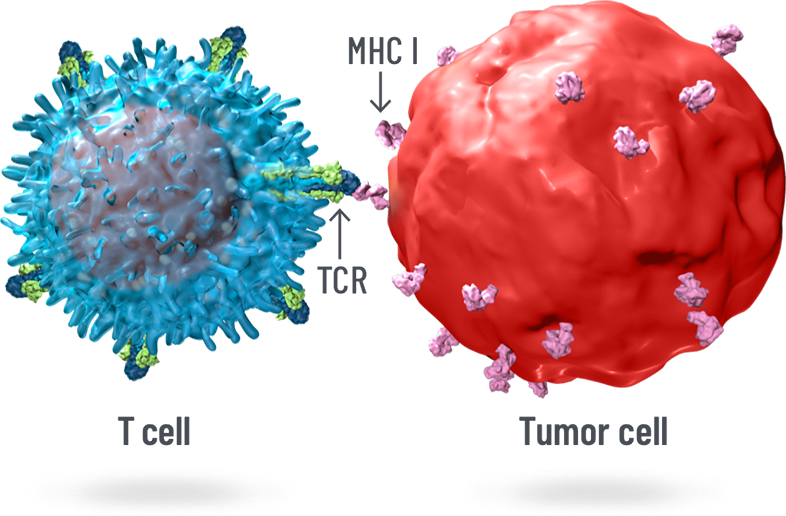
Cytotoxic T cells may recognize cancer cells via TCR-MHC I binding, which can result in T-cell–mediated tumor cell lysis11
Tumors can evade immune detection by downregulating MHC I and through an immunosuppressive tumor microenvironment12
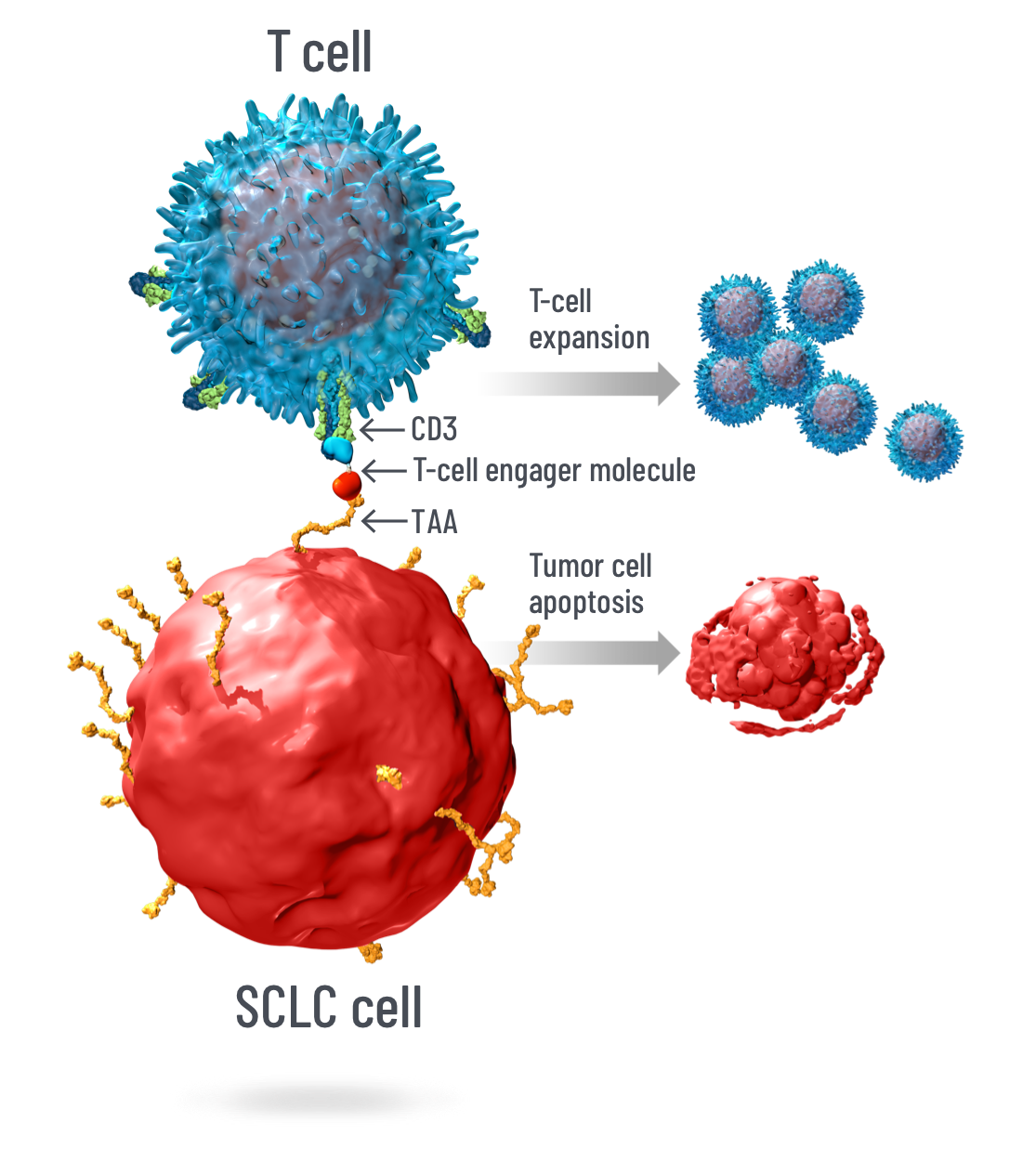
Investigational T-cell engagers may be designed to target DLL3-expressing tumor cells in SCLC and other high-grade NECs5
-
TCEs are designed to bind both a tumor-associated antigen, such as DLL3, on tumor cells and CD3 on T cells1
-
They create an immunological synapse, or T-cell–mediated immunity, between T cells and tumor cells, and can activate T cells13
-
Activated T cells may induce apoptosis of tumor cells and proliferate locally, resulting in expansion of T cells that facilitate additional T-cell–dependent killing13
Have questions about DLL3, TCE technology, and their potential roles in treating SCLC?
CD, cluster of differentiation; MHC I, major histocompatibility class I; TAA, tumor-associated antigen; TCE, T-cell engager; TCR, T-cell receptor.
Resources on DLL3 and TCE technology in SCLC:
Videos
A Powerful Connection
See oncologist Dr Eric Schaefer discuss the potential of investigational DLL3-targeted T-cell engager technology
0:07Dr Eric Schaefer: Hi, I’m Dr Eric Schaefer, and I’m a medical oncologist/hematologist at Highlands Oncology in Northwest Arkansas.
0:15Dr Eric Schaefer: So, what do we know about small cell lung cancer today?
0:19Dr Eric Schaefer: Small cell lung cancer is a devastating and aggressive high-grade neuroendocrine cancer, which will account for an estimated 30,000 new cases in the United States in 2023 alone.
0:30Dr Eric Schaefer: ;About two-thirds of patients with small cell lung cancer are diagnosed with extensive-stage disease, which is associated with especially poor prognosis, and a median survival of 10–13 months.
0:42Dr Eric Schaefer: Over the last few decades, there have only been a few treatment advances for small cell lung cancer. In 2019 and 2020, two anti–PD-L1 checkpoint inhibitors in combination with platinum-based chemotherapy were FDA-approved for the treatment of first-line extensive-stage disease. However, additional treatment options are needed.
1:04Dr Eric Schaefer: And while immune checkpoint inhibitors have significantly changed the treatment paradigms across multiple other cancer types, it has seen limited success in small cell lung cancer. Lastly, if we look beyond the first-line setting, there are two FDA-approved therapies in the second-line setting, but there is no standard-of-care in or after the third-line setting. For this reason, there remains a need for new, innovative therapies with durable benefits for patients with small cell lung cancer. Exciting advancements are taking place in the small cell lung cancer research landscape.
1:38Dr Eric Schaefer: So, why is DLL3 an exciting target in the advancement of small cell lung cancer treatment?
1:44Dr Eric Schaefer: In oncology, our goal is to treat the cancer cells, while minimizing effects on normal cells. In order to do this, a drug should target receptors that are more highly expressed in tumor tissue than in healthy tissue. Delta-like ligand 3, or DLL3, is an exciting potential target in small cell lung cancer for this very reason.
2:03Dr Eric Schaefer: It is important to note that the biologic function of DLL3 is not completely understood.
2:10Dr Eric Schaefer: But what we do know is that DLL3 is an inhibitory protein of Notch signaling, a pathway involved in embryonic development and neuroendocrine cell differentiation. DLL3 is involved in tumor progression of neuroendocrine malignant neoplasms, and an increased expression may be associated with poor survival.
2:29Dr Eric Schaefer: In healthy cells, DLL3 is typically located in the Golgi apparatus and cytoplasmic vesicles, and is rarely found on the cellular surface.
2:38Dr Eric Schaefer: But in high-grade neuroendocrine tumors like small cell lung cancer, DLL3 is expressed on the cell surface.
2:46Dr Eric Schaefer: In fact, a large, multicenter study found that 85% of patients with small cell lung cancer had positive DLL3 expression. And this was consistent across disease stages—83% of patients with limited-stage disease and 86% of those with extensive-stage disease had positive DLL3 expression.
3:07Dr Eric Schaefer: In the same study, the proportion of patients with small cell lung cancer with positive DLL3 expression remained consistently high across lines of therapy.
3:17Dr Eric Schaefer: This high expression on the surface of small cell lung cancer and high-grade neuroendocrine cancer cells and minimal expression on normal cells makes DLL3 an exciting target, particularly for those investigational T-cell engager technology.
3:32Dr Eric Schaefer: So, how is investigational T-cell technology designed to target DLL3?
3:37Dr Eric Schaefer: Cytotoxic T cells may play an important role in recognizing and fighting tumor cells.
3:42Dr Eric Schaefer: They help recognize cancer cells via T-cell receptor–major histocompatibility complex one, or MHC I. Once bound, this can result in T-cell–mediated tumor cell lysis.
3:54Dr Eric Schaefer: But tumors can evade immune detection through various mechanisms to help them survive and proliferate.
3:59Dr Eric Schaefer: These include: Downregulation of the MHC I complex, inhibition of the T-cell receptor signaling, use of the PD-1 or PD-L1 signaling pathway, and the formation of an immunosuppressive tumor microenvironment.
4:14Dr Eric Schaefer: In the case of small cell lung cancer, it is known as being an immunologically "cold tumor" with few infiltrating cytotoxic T cells. This is where investigational T-cell engagers hope to come into play––they're designed to target DLL3-expressing tumor cells such as small cell lung cancer and other high-grade neuroendocrine cancers.
4:34Dr Eric Schaefer: Investigational T-cell engagers are designed to bind to both a tumor-associated antigen such as DLL3 on tumor cells, and CD3 on T cells, creating a cytolytic synapse, potentially activating T cells. Activated T cells release lytic granules containing perforin which inserts into the target cell membrane creating pores,
4:57Dr Eric Schaefer: allowing for the transfer of granzymes, which may induce apoptosis of the tumor cells. Activated T cells may also proliferate, resulting in expansion of T cells to facilitate additional T-cell–dependent killing.
5:10Dr Eric Schaefer: As such, T-cell engager technology may provide a powerful connection, potentially redirecting cytotoxic T cells to target and fight small cell lung cancer.
5:20Dr Eric Schaefer: In summary, small cell lung cancer is a devastating disease and there's a high unmet need for these patients. Highly expressed on the surface of small cell lung cancer cells and minimally expressed on normal cells, DLL3 is an exciting possible target. Investigational T-cell engagers have a potential to provide a powerful connection, directing the patient's own T cells to target DLL3-expressing tumor cells in small cell lung cancer. All in all, DLL3 and T-cell engager technology have intriguing potential to advance the small cell lung cancer treatment paradigm.
5:56Dr Eric Schaefer: Thank you for tuning in. To learn more, visit DLL3Possibilities.com.
Overview of SCLC and TCEs
TCEs targeting DLL3 in SCLC and other neuroendocrine cancers
0:06Voiceover: Cytotoxic T cells play an important role in recognizing and fighting cancer cells.
0:13Voiceover: The T-cell receptor (TCR) binds to peptides presented by major histocompatibility complex class I (MHC I) on cancer cells, which can result in cancer cell lysis.
0:26Voiceover: However, cancer cells can develop mechanisms to evade T-cell recognition.
0:32Voiceover: One mechanism is the downregulation of MHC I on the cancer cells that can result in an immunosuppressive microenvironment.
0:42Voiceover: T-cell engagers are designed to direct the patient's own T cells to target cancer cells.
0:48Voiceover: They are designed to bind T cells to cancer cells without relying on MHC recognition.
0:58Voiceover: Bispecific T-cell Engager, or BiTE® technology, is a T-cell engager platform.
1:04Voiceover: BiTE® molecules consist of a domain that is designed to bind a tumor-associated antigen on cancer cells, and a domain that binds CD3 on T cells.
1:19Voiceover: They can also contain a silenced Fc domain for an extended half-life.
1:25Voiceover: Amgen is investigating BiTE® molecules against different targets.
1:30Voiceover: In small cell lung cancer, Amgen developed a BiTE® molecule with the goal of targeting delta-like ligand 3, or DLL3.
1:39Voiceover: DLL3 is an inhibitory Notch pathway ligand involved in embryonic development and neuroendocrine cell differentiation.
1:47Voiceover: In healthy cells, DLL3 is typically located in the Golgi apparatus and cytoplasmic vesicles.
1:55Voiceover: It is rarely found on the cell surface.
2:00Voiceover: In SCLC and other high-grade neuroendocrine cancers, DLL3 is localized on the cell surface, making it an attractive target for targeted immunotherapy using BiTE® technology.
Downloads

About DLL3
A fact sheet that highlights the biology of DLL3 and its potential as a target for investigational TCE technology in SCLC and other high-grade NECs
About DLL3
A fact sheet that highlights the biology of DLL3 and its potential as a target for investigational TCE technology in SCLC and other high-grade NECs
Harnessing the Potential of T Cells and DLL3 in SCLC
A medical disease state education resource that overviews the unmet need in SCLC and how DLL3 is a potential target for emerging investigational TCE technology

Harnessing the Potential of T Cells and DLL3 in SCLC
A medical disease state education resource that overviews the unmet need in SCLC and how DLL3 is a potential target for emerging investigational TCE technology
Helpful Links
Amgen continues its commitment to patients by advancing all angles of care for tough-to-treat cancers.
Learn more
Additional information on DLL3 is available.
Discover more
-
References: 1. Einsele H, et al. Cancer. 2020;126:3192-3201. 2. Sabari JK, et al. Nat Rev Clin Oncol. 2017;14:549-561. 3. Paz-Ares L, et al. Lancet. 2019;394:1929-1939. 4. Horn L, et al. N Engl J Med. 2018;379:2220-2229. 5. Owen DH, et al. J Hematol Oncol. 2019;12:61. 6. Rudin CM, et al. Nat Rev Dis Primers. 2021;7:3. 7. National Cancer Institute. www.cancer.gov. Accessed February 14, 2023. 8. Leonetti A, et al. Cell Oncol (Dordr). 2019;42:261-273. 9. Rojo F, et al. Lung Cancer. 2020;147:237-243. 10. Ahn MJ, et al. N Engl J Med. 2023. doi:10.1056/NEJMoa2307980. 11. Baeuerle PA, et al. Curr Opin Mol Ther. 2009;11:22-30. 12. Yuraszeck T, et al. Clin Pharmacol Ther. 2017;101:634-645. 13. Nagorsen D, et al. Exp Cell Res. 2011;317:1255-1260.